No
Purpose
Rural Health Transformation Program (RHTP) Health Care Advisory Regions (HCARs) are established to provide structured, region-specific health care insight and coordinated input to the RHTP. The HCARs ensure that RHTP initiatives are informed by local health care delivery realities, workforce conditions, infrastructure capacity, and community needs, while remaining aligned with statewide priorities and the Nebraska Department of Health and Human Services (DHHS) program requirements.
Six HCARs will be established across the state to ensure consistent, geographically grounded engagement and strengthen two-way communication among DHHS, providers, and regional stakeholders.
Role in the Governance Model
HCARs serve as formal advisory and engagement bodies within the RHTP governance structure. They do not function as approving authorities. Instead, they provide organized regional input, recommendations, and implementation perspectives to DHHS and RHTP.
HCARs support DHHS in:
- understanding regional variation in needs and readiness,
- identifying opportunities for collaboration and sequencing, and
- anticipating implementation risks and unintended impacts.
Final decision-making authority remains with DHHS in accordance with federal, state, and CMS requirements.
Composition & Membership Structure
Regional Structure
- Six HCARs are aligned to defined geographic boundaries and rural economic development regions.
- Each region includes both voting and non-voting members to balance formal representation with broad subject-matter expertise.
Voting & Non-Voting Members
- Voting members represent defined provider types and stakeholder categories critical to regional health care delivery.
- Non-voting members provide subject-matter expertise, implementation insight, or cross-sector perspective.
A standardized list of eligible provider types for voting and non-voting participation will be maintained by DHHS.
| Representation | Voting Member | Notes |
| Rural Prospective Payment System Hospital | Yes | The Southeast Region does not have a rural PPS hospital. |
| Critical Access Hospital / Rural Emergency Hospital | Yes | Northeast, Central, Mid-Plains, and Western Regions - 2 CAHs (or REH) – one must be independent, and the other may be independent or system-owned
|
| | | Southeast Region - 3 CAHs (or REH) – one must be independent, and the other two may be independent or system-owned
|
| | | Metro Region |
| Hospital-Owned Medical Clinic | Yes | |
| Private Practice Medical Clinic | Yes | |
| Nursing Facility / Skilled Nursing Facility | Yes | |
| Assisted Living Facility | Yes | |
| Emergency Medical Services – Hospital-based | Yes | Selected through a DHHS application process. |
| Emergency Medical Services - Community or County-based | Yes | Selected through a DHHS application process. |
| Dental Provider / Dental Practice | Yes | |
| Federally Qualified Health Center | Yes | |
| Behavioral Health – Independent Provider | Yes | |
| Certified Community Behavioral Health Clinic | No | |
| Local Health Department | No | |
| Pharmacy Provider | No | |
| Ancillary Healthcare Provider (e.g., optometry) | No | Selected through a DHHS application process. |
| Home Health Agency | Yes | |
| Community College | No |
|
Become a Member
- Provider Associations will coordinate with their membership to identify and nominate representatives for each HCAR except the ancillary provider and EMS representatives. Those representatives will be selected through a DHHS-managed application process.
- DHHS will confirm appointments to ensure balanced regional representation and alignment with governance expectations.
- Members serve in a regional advisory capacity and represent system-level perspectives rather than individual organizational interests.
- The Ancillary Healthcare Provider and Emergency Medical Services representatives will be selected through a DHHS-managed application process.
- Provider Association Member Contact Information
Application Process
For the EMS Representatives:
Definition – Emergency Care Provider is a Nebraska-licensed Emergency Medical Technician (EMT), Advanced Emergency Medical Technician (AEMT), or Paramedic who is actively involved in the provision of pre-hospital emergency medical care on a Nebraska-licensed Emergency Medical Service (EMS) that responds to 100 or more calls per year.
Application Process - Health Care Advisory Region (HCAR) applicants can download a fillable PDF application form and email it to DHHS.RHTP@nebraska.gov.
Applications Due: April 14, 2026
Criteria - For an application to be considered, a provider must meet the following criteria.
- Must have been in practice for no less than three years
- Must be located in the region that is being applied for and currently practicing in a rural setting
- Must be employed or volunteer for a Nebraska-licensed EMS
Selection Process - DHHS will convene an application review committee to review applications and officially select members of the HCAR. DHHS will inform applicants via email that they have been selected to serve on the HCAR. Upon the applicant's acceptance, they will be confirmed as members of the HCAR.
Applications will be assessed for:
- The geographic needs of the region
- Relevance of the applicant's skills and experience
- Clarity and relevance of the applicant's written responses
- The types of EMS experience and leadership the applicant has
- The scarcity of the EMS services and hospital partners available in the applicant's service area
- The amount of practice experience that the applicant has
Ancillary Provider Representative:
Definition - An ancillary healthcare provider is a medical entity or professional that offers supportive and diagnostic services to supplement the primary care provided by doctors, nurses, or hospitals. For the purposes of HCAR, it means a provider of the following services.
- PT/OT/ST
- Audiology
- Optometry
- Medical Nutrition Therapy
- Podiatry
- DME
- Chiropractic
- Respiratory therapy
- Social work
- Radiology
- Lab
Application Process - Health Care Advisory Region (HCAR) applicants can download a fillable PDF application form and email it to DHHS.RHTP@nebraska.gov.
Applications Due: April 14, 2026
Criteria - For an application to be considered, a provider must meet the following criteria:
- Must have been in practice for no less than three years
- Must be local to the region that is being applied for and have practiced or currently be practicing in a rural setting
- Must either be employed by a Critical Access Hospital (CAH) or an independent practitioner
Selection Process - DHHS will convene an application review committee to review applications and officially select members of the HCAR. DHHS will inform applicants via email that they have been selected to serve on the HCAR. Upon the applicant's acceptance, they will be confirmed as members of the HCAR.
Applications will be assessed for:
- The geographic needs of the region
- Relevance of the applicant's skills and experience
- Clarity and relevance of the applicant's written responses
- The types of ancillary services the applicant provides
- The scarcity of the services being provided by the applicant
- The amount of practice experience that the applicant has
Key Responsibilities
HCARs are responsible for providing structured, actionable regional input to support effective RHTP implementation, including:
- Identifying regional health care access, workforce, and infrastructure needs.
- Providing a regional perspective on initiative readiness, feasibility, and sequencing.
- Offering recommendations on how initiatives may be tailored to regional conditions.
- Supporting coordination among regional providers, partners, and stakeholders.
- Identifying emerging challenges, risks, and opportunities during implementation.
- Communicating observed regional impacts and outcomes back to DHHS.
Engagement Mechanisms & Cadence
- HCARs will meet every other month during initial implementation, with the option to adjust cadence as the program matures.
- Meetings will follow Open Meetings Act requirements, which include providing a standardized agenda and formal input opportunities. Additionally, meeting materials, such as minutes and handouts, will be maintained online to ensure transparency and continuity.
- Engagement mechanisms may include:
- Structured regional input sessions
- Written recommendation summaries
- Participation in initiative-specific or time-limited workgroups
Relationships with Other Governance Bodies
- HCARs provide structured input to DHHS through defined channels.
- Regional insights may be elevated to the Rural Health Advisory Commission (RHAC) to inform statewide stakeholder discussions.
Transparency & Accountability
HCAR activities and input are part of RHTP's broader transparency and stakeholder engagement strategy. DHHS will communicate how regional input is considered and, when recommendations are not adopted, provide a rationale as appropriate.
Meetings
Initial HCAR Meeting Information: View the agenda for these meetings.
- Central Region
- Wednesday June 17, 2026: 1:00pm – 4:00pm (Central Time - Chicago)
- Home Federal Bank, 3311 W Stolley Park Rd, Grand Island, NE 68803, USA
- Southeast Region
- Thursday June 18, 2026: 1 PM – 4 PM
- Nebraska Department of Health and Human Services Administrative Offices, 301 Centennial Mall S, Lincoln, NE 68508, USA
- Mid-Plains Region
- Monday, June 22, 2026: 1:30 PM-4:30 PM
- Great Plains Health, 601 W Leota St, North Platte, NE 69101, USA
- Western Region
- Tuesday, June 23, 2026: 1:00 PM-4:00 PM
- Prairie Winds Community Center, 428 N Main St, Bridgeport, NE 69336, USA
- Northeast Region
- Thursday, June 25, 2026: 1:00 PM-4:00 PM
- Faith Health, South Medical Office Building, 2701 W Norfolk Avenue, Norfolk, NE 68701, USA
- Metro Region
- Friday, June 26, 2026: 1:00 PM-4:00 PM
- Health Park Plaza, 450 E 23rd St, Fremont, NE 68025, USA
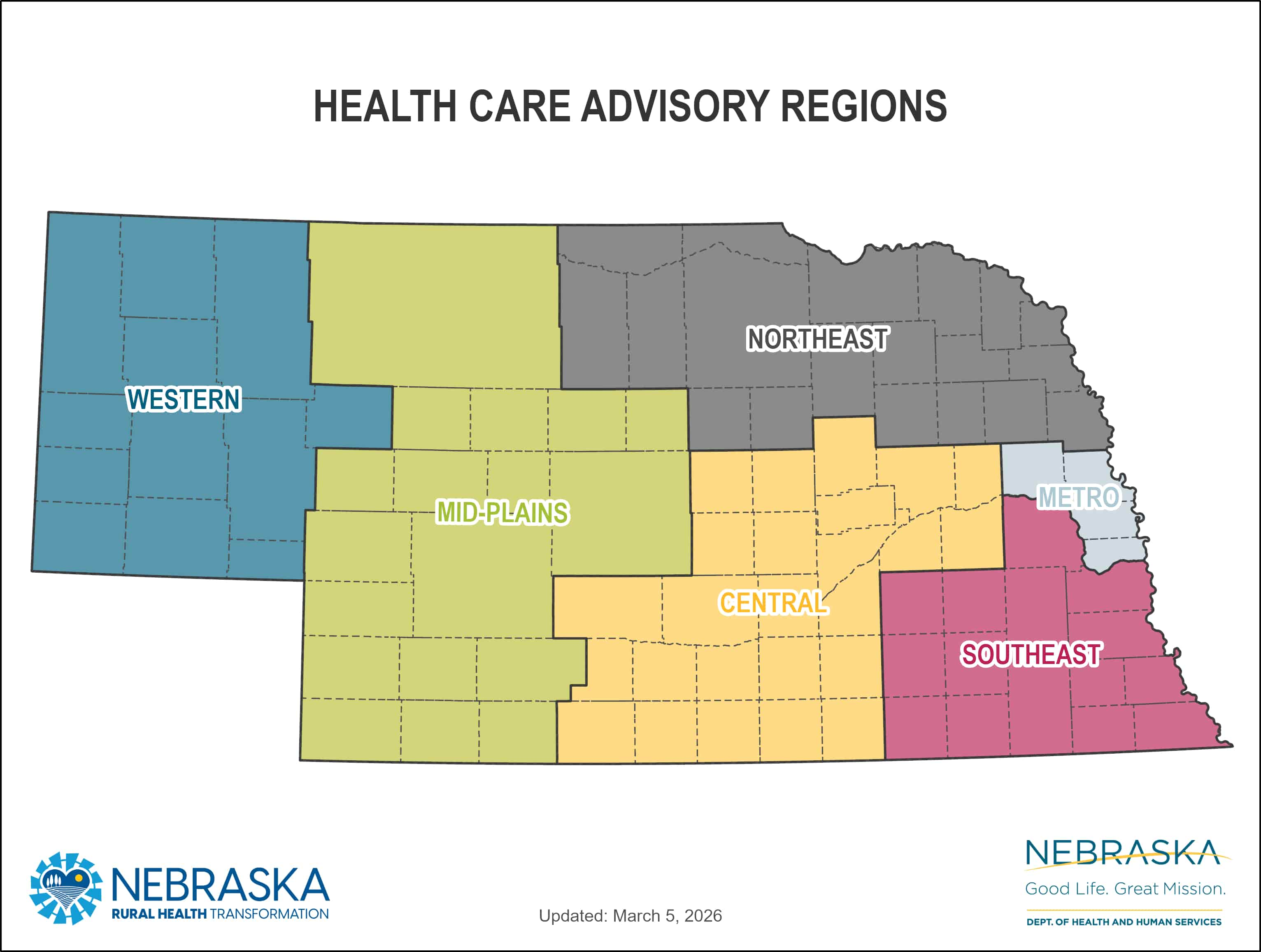
Regions Map
The following map illustrates the six RHTP HCARs, aligned to defined geographic boundaries to ensure structured, region-specific engagement across the state.
 View an accessible PDF.
View an accessible PDF.
The Rural Health Transformation Program is supported by the Centers for Medicare & Medicaid Services (CMS) of the U.S. Department of Health and Human Services (US HHS) as part of a financial assistance award totaling $218,529,075.01 with 100 percent funded by CMS/US HHS. The contents are those of the Nebraska Department of Health and Human Services (DHHS) and do not necessarily represent the official views of, nor an endorsement by, CMS/US HHS, or the U.S. Government.